
Changing a voice prosthesis
Depending on the make, the lifetimes of the currently available indwelling voice prostheses range from weeks to months. That is why the prostheses have to be replaced at regular intervals. This is usually effected through the tracheostoma with the patient awake, and having been given local anesthesia if desired. Just how demanding changing the voice prosthesis is for the patient and for the doctor depends on how many times it has already been changed, the size of the tracheostoma, where the esophagotracheal fistula is, what method of insertion was used, whether there are any complications to control, and how sensitive the patient is to manipulation of the wind pipe.
The band width ranges from unproblematic replacement with the same type of voice prosthesis that takes just a few seconds, to an extremely dynamic procedure on a non-anaesthetized patient who could be coughing or vomiting and at risk of aspiration. Besides replacement of the voice prosthesis, the sizing of the correct prosthesis length, recanalisation of the esophagotracheal fistula, and even a new puncture may become necessary without prior warning.
The following is a proven method for changing a voice prosthesis which can, of course, be significantly modified and shortened, depending on the patient, situation and the surgeon's level of experience.
Some fundamental requirements regarding the external conditions for changing a voice prosthesis need to be observed. A headlight or adjustable light should be available so the operator has both hands free. There must also be sufficient light in the tracheostoma. Whether an existing tracheostoma aadhesive needs to be removed depends on whether a dilator needs to be fixed, how far the tracheostoma is and how far down the voice prosthesis is located.
A) Preparation
Patients do not always come specifically to have their voice prosthesis changed. Often, they are seeking advice regarding a problem that could possibly be solved by changing the voice prosthesis. The problem that most often leads to a change of the voice prosthesis is leaking. One typical example of this is the coffee that the patient has either coughed up or sucked out of the wind pipe. A faulty valve in the voice prosthesis may have allowed the coffee to run through the voice prosthesis (transprosthetically) into the wind pipe. This problem can be solved by changing the voice prosthesis. However, the coffee could also have got past the voice prosthesis (periprosthetically) into the wind pipe due to an expansion of the esophagotracheal fistula. If this happens, the problem often cannot be solved simply by replacing the voice prosthesis with the same model.
1) The most important criterion in the decision is the type of leak
periprosthetic (past the prosthesis) or transprosthetic (through the prosthesis). The leak is checked by a swallow test before changing the voice prosthesis. So the swallow test serves less to confirm the patient's claim that the prosthesis is leaking, than to provide a more detailed analysis of the problem. A transprosthetic leak is usually rectified by changing the voice prosthesis. Once it has occurred, even intensive cleaning will generally not help to achieve permanent valve closure.
In the simplest case, a periprosthetic leak may be caused by the voice prosthesis being too long, which is easy to remedy. It can also be caused by atrophy and dilation of the shunt or an infection and necrosis around the shunt, which are not quite so easy to deal with.
Management of a periprosthetic leak
The swallow test to differentiate between transprosthetic and periprosthetic leakage: water is usually used for the swallow test, as this is the least risky in the event of aspiration. It is rare for a colored liquid (e.g. water with a little milk, water with methylene blue etc.) to be required to determine minor leaks. The patient should drink a normal mouthful of water at least three times. The patient will make a number of smaller swallows after the first one; here too, check for signs of leakage. Any liquid that escapes is to be sucked up to prevent aspiration. Transprosthetic leakage is usually easy to diagnose. Leakage around the voice prosthesis may be difficult to see.
Leakage (Video)
Inspection of the esophagotracheal fistula also provides information on the possibility of periprosthetic leakage. Tear-shaped shunts or shunts with visible signs of infection or even necroses are often indications of periprosthetic leakage.
2) The length of the prosthesis
is the second important criterion that should at least be considered before changing the prosthesis. If the inserted prosthesis is neither too long nor too short, then the new prosthesis should be of the same length. If the length needs to be adjusted, then the length of the old prosthesis will serve for guidance. The exact length of the new prosthesis should then be measured with a measuring device once the old prosthesis has been removed. It is important to know that the shunt needs to be measured, as changing the voice prosthesis must now include an interim step, the measuring, and the appropriate instruments and prostheses of various lengths need to be available.
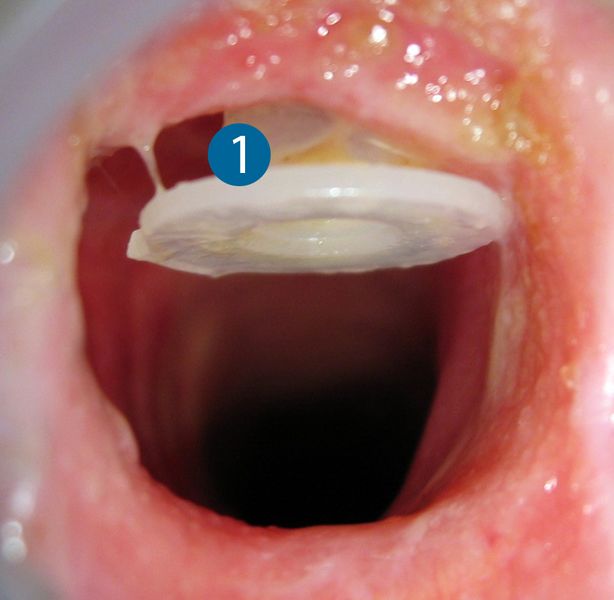
A voice prosthesis (1) that is more than 2 mm too long should be replaced by a shorter one, as otherwise it could move around in the shunt like a piston, causing a periprosthetic leak. Under no circumstances is a prosthesis that is too short to be used, as it may cause circulatory problems in the shunt that could result in permanent damage. A well-fitting voice prosthesis will be positioned perfectly without exerting pressure, or will have up to 2 mm leeway.
3) The choice of prosthesis
is the third criterion that needs to be considered before changing the voice prosthesis. If the prosthesis that has been used so far has been in-situ for long enough, the patient was happy with it and there are currently no problems on the shunt, then the same prosthesis model should be used. If the lifetime of the prosthesis is once again (too) short, there is a significant amount of biofilm on the valve, there is evidence of underpressure related valve openings when inhaling or there are problems with the shunt, then the use of a special prosthesis should be considered.
4) Method of insertion
Once the choice of prosthesis has been made, the suitable method of insertion is decided upon. The first to be considered is the method of insertion recommended by the manufacturer of the particular prosthesis. A different method of insertion may be chosen if there are valid reasons for doing so. Almost all voice prostheses can be e.g. changed retrograde by means of a guide wire through the mouth if this is necessary.
You will find a detailed presentation of the advantages and disadvantages of the various methods at:
5) Preparation and provision of instruments
It has proved worthwhile to provide the instruments required for changing a voice prosthesis in a set, since it is not always easy to find the required instruments while the change is underway.
B) Changing the voice prosthesis
While the voice prosthesis is being changed, aspiration of saliva must be prevented as otherwise it could lead to disturbances from coughing. If the shunt is not sealed by a prosthesis or dilator, the patient is to be asked to open his mouth wide. Most people are unable to swallow if their mouth is wide open, which will help to prevent the aspiration of swallowed saliva while changing the prosthesis. This is of particular importance, since laryngectomees are able to swallow and inhale simultaneously.
It is unusual to have to use an anesthetic spray on the tracheal membranes to reduce pain and coughing when changing the voice prosthesis.
1) First, the old voice prosthesis is removed. Ideally, clamp the tracheal flange with two anatomical clamps and pull it right out of the shunt. Once the prosthesis has been removed, seal the shunt immediately by inserting a dilator.
2) If the length of the shunt needs to be measured, remove the dilator and insert a measuring device; perform the measurement and reinsert the dilator.
3) Now insert the prosthesis using the chosen method of insertion.
4) Check the function of the voice prosthesis once it has been inserted. The patient checks to see whether speech works. This is followed by another swallow test to check the seal of the prosthesis.
5) When all the functions are as required, check the correct position of the voice prosthesis in the shunt. The prosthesis should turn slightly (not Eska-Herrmann prostheses) and the esophageal flange should be positioned safely in the food pipe. If there is any doubt, then an endoscopic check of the correct position of the prosthesis is recommended.
6) If the function and position of the voice prosthesis are correct, the retaining tape of indwelling prostheses can be cut. Some manufacturers recommend turning the prosthesis into a special position once the retaining tape has been trimmed.

Changing a voice prosthesis (video)
If the correct position of the esophageal flange is to be checked, the safest way to do this is by transprosthetic endoscopy. An endoscope will fit through most prostheses, and the esophageal flange can be checked by sight in the food pipe.
C) Follow-up
Following up the changing of the voice prosthesis includes:
- Patient instruction (type of prosthesis, caring for the prosthesis etc.)
- Care of the tracheostoma (tubes, adhesives etc.)
- Documentation of the type of prosthesis and any special considerations
- Patient motivation to use an HME