Surgical shunt creation by puncture and spacer
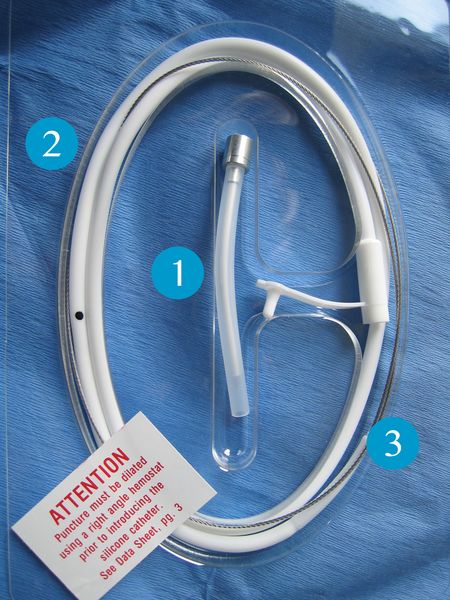
The Blom-Singer® Tracheoesophageal puncture set can be used both for primary and secondary creation of an esophagotracheal fistula. It consists of a soft silicone stomach tube (2) with a soft, flexible wire (3) secured to the top and a slightly bent, stable cannula (1) through which the wire passes.
This set is used to place a shunt where the stomach tube will remain as a spacer until the shunt has stabilized. After a week, once the initial swelling has worn off, the stomach tube is removed, the shunt measured and the suitable voice prosthesis inserted. This concept may be advantageous to patients where there is a risk of delayed wound healing (radiation patients) as there is no risk of pressure necroses on the newly created shunt caused by the flanges of the voice prosthesis.
The use of the Blom-Singer® Tracheoesophageal puncture set is demonstrated in the following on a surgical model (no laboratory animals involved)

Puncture of the Pars membranacea exactly in the midline 1 cm caudal of the upper edge of the tracheostoma into the esophagus.
The puncture cannula on the inside is removed after the puncture.
The plastic outer cannula is left in-situ.

The wire is now pushed into the esophagus through the outer plastic cannula.

When the wire is visible in the open pharynx, it is grasped there and pulled through the puncture site by the attached conical stomach tube.

The plastic outer tube is also pulled through the shunt.

Once the stomach tube has been pulled through far enough, the conical tip and wire are cut off. This opens the lumen on the tube. The tube is now pushed to caudal in the esophagus, and its correct position checked by auscultation.
It is then stitched to the tracheostoma.
The patient is fed via this tube for between one and two weeks, depending on the progress of healing (this has the added advantage of not necessitating a nasogastric tube). The tube is then removed and a voice prosthesis inserted anterograde in the stabilized shunt.