Myotomy and neurectomy
In order to speak using a voice prosthesis, air must flow from the wind pipe through the voice prosthesis into the food pipe and from there up into the mouth.
The flow of food or air in the pharynx upwards into the mouth is unphysiological, and is usually prevented by strong contractions of the pharyngeal muscles (M. constrictor pharyngis). In order to prevent the contraction of the pharyngeal muscles when air flows through the voice prosthesis and upwards for TE-speech, the pharyngeal muscles must be cut on one side (myotomy).
As even only a few remaining muscles fibers could make talking far more difficult, the pharyngeal constrictor muscle (M. constrictor pharyngis) must be cut through very carefully and completely without damaging the mucus membrane beneath it, as otherwise leaking saliva will impede the healing process.
There are several versions of myotomy: dorsal, medial and unilateral. Dorsal myotomy runs along the midline of the dorsal esophageal entry to the upper hypopharynx. It is carried out using a Sengstaken tube, and is laborious.
If a medial myotomy is carried out (separation of the pharyngeal constrictor in the middle) and comes close to the voice prosthesis, this may weaken the esophagotracheal fistula (subsequent tear-shaped deformation) and cause leaking around the prosthesis.
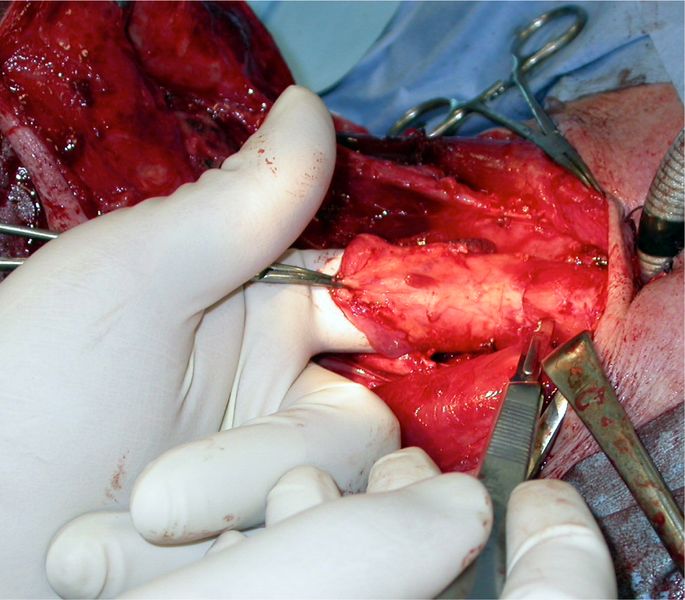
In our hands the myotomy of the M. constrictor pharyngis is ideally carried out along one side (unilateral), starting at the voice prosthesis and running along the entire hypopharynx to the base of the tongue. The unilateral myotomy is easier to perform than the dorsal myotomy, is extremely effective, and there is no risk of weakening of the esophagotracheal fistula.
In addition to the myotomy of the M. constrictor pharyngis, the unilateral neurectomy (nerve separation) of the Plexus pharyngis, which innervates the pharyngeal muscles, has proved successful. If the two procedures are combined, it is extremely rare for a pharyngeal spasm (pharyngospasm) to block the speech flow.
For the neurectomy, the nerve fibers of the pharyngeal plexus, which radiate from lateral into the pharyngeal muscles, are separated to the level of the tonsil. This measure extends the operation by only a few minutes, but significantly increases the chances of successful voice rehabilitation.
Myotomy and Neurectomy
If, despite all surgical endeavors, a pharyngeal spasm ever inhibits speech, then an EMG-controlled injection of Botulinum toxin will generally still help to achieve a good level of speech. Secondary myotomy is not recommended because of the high risk of complications.