Instruments for secondary shunt creation
There are no standardized surgical instruments available for secondary placement of a voice prosthesis. Scars and pharynx stenosis in particular can make secondary placement of a voice prosthesis more difficult. Techniques using flexible endoscopy for secondary placement of a voice prosthesis performed while the patient is awake have been described. However, they are only successful if the conditions are ideal (wide pharynx, large tracheostoma, tolerant patient).
The following procedure under general anesthetic has proved the most successful:
1. Rigid endoscopic presentation of the neopharynx and entrance to the esophagus to rule out scarred stenoses. As the pharynx is not open, unlike during laryngectomy, the pharynx protector cannot be used. Instead, a rigid endoscope (1) is pushed into esophagus until it lies about 1 cm caudal of the top edge of the tracheostoma.
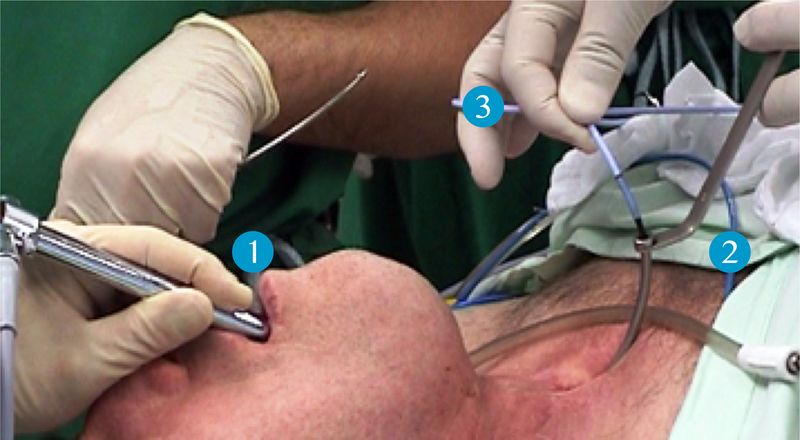

The correct position of the rigid endoscope is checked by palpation. This is followed by puncture with the trocar after Hilgers into the lumen of the endoscope. When the tip of the trocar is visible in the endoscope, the trocar is removed and the outer tube (2) pushed a little further into the endoscope so it is safely positioned. A guide wire (3) can now be pushed into the endoscope. The endoscope is removed, as is the outer tube. The guide wire is pulled out of the mouth and a voice prosthesis attached to it. The voice prosthesis is drawn into the shunt by the guide wire, and unfolded there.
If there is a scarred tightening of the neopharynx that prevents a large lumen rigid endoscope from being inserted, then the procedure will have to be modified:
Option 1: Under certain circumstances, a scarred pharynx stenosis can be stretched a little using dilators (3), so a rigid endoscope can still be used to display a suitable puncture point for the trocar after Hilgers.
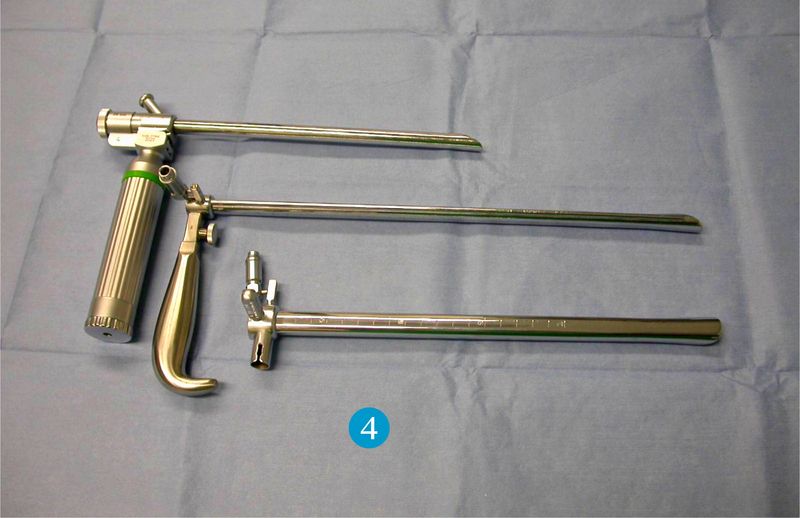
Option 2: Often, a small lumen endoscope (4) can be used to display a suitable puncture point in the esophagus. If the puncture trocar after Hilgers does not fit in the small lumen endoscope, then the puncture can be made with a standard injection needle instead. The needle is used to draw a stable thread, e.g. Mersilene 2.0, into the endoscope. The thread is then pulled out the endoscope using forceps. The endoscope is now removed and a voice prosthesis tied firmly to the thread. The voice prosthesis is now drawn into the puncture by the thread and unfolded there using small anatomical clamps.